















 792 844
792 844

3.
Evidence synthesis
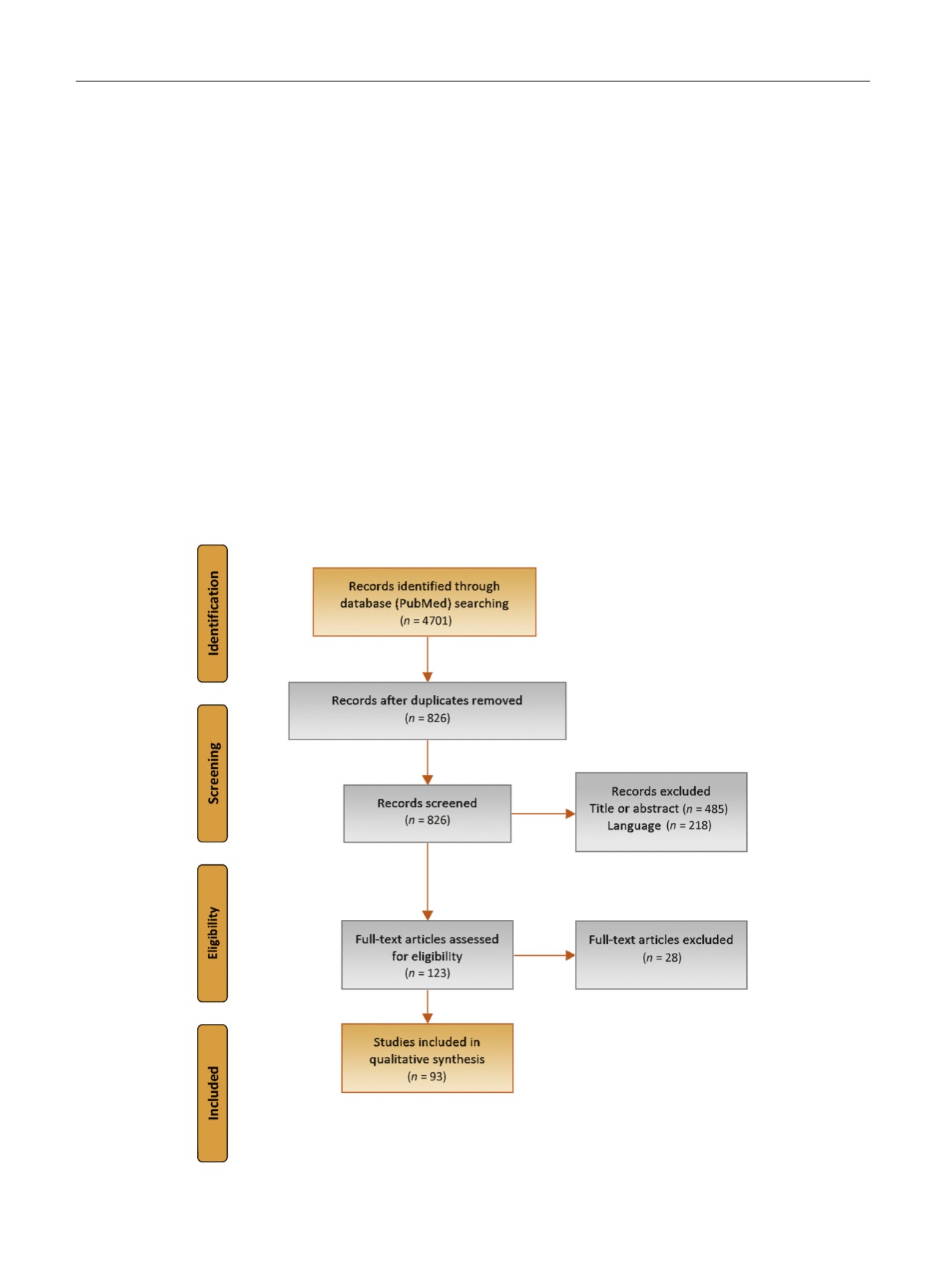
The search revealed 116 studies eligible for inclusion in the
review. Of these, 93 were finally included
( Fig. 1 ). Given the
characteristics of the studies included and the heterogene-
ity of the available articles in terms of methodology, no
meta-analysis was attempted.
3.1.
Pathogenesis of BE
3.1.1.
Anatomic arguments and studies on the frequency of
association of the different forms
As a general overview, it has to be mentioned that on one
hand, DIE nodules are thought to originate as the natural
evolution of superficial peritoneal endometriosis infiltrat-
ing behind the peritoneum, while on the other, they are
thought to be adenomyotic nodules originating via a
process of metaplasia
[13]. Specifically for the bladder,
the distribution of lesions in relation to factors influencing
the spreading of endometrial cells supports the pathoge-
netic theory of spontaneous BE on the basis of implantation
of transtubally regurgitated menstrual endometrium
on peritoneal surfaces. Owing to gravity, the anterior
cul-de-sac where the bladder is located represents the
most frequent site. After implantation, the underlying
inflammatory process favors the development of adhesions
between the contiguous organs and the formation of a
fibrotic nodule, apparently of the vesicovaginal septum,
that is buried under the peritoneum
[14,15]. Anatomic
observations strongly supporting this theory include the
absence of BE in women with a retroverted uterus, in whom
an anterior cul-de-sac is not present, and the location of
most nodules adherent to the uterine body well above the
uterine isthmus, adherent to the anterior uterine wall, if not
the fundus
[15]. Support for this theory comes from studies
evaluating the frequency of association between the
different forms of the disease, on the assumption that if a
peculiar pathogenetic mechanism leading to a specific form
of the disease exists, the frequency of other forms of
endometriosis in patients affected by the peculiar form
should be similar to the frequency observed in the general
population (prevalence 4%
[16]). Among cases affected by
BE, the incidence observed was 58.6% (95% confidence
interval [CI] 45.2–71.2) for superficial peritoneal implants,
44.8% (95% CI 32.2–58.2) for ovarian endometriomas,
81.0% (95% CI 68.4–89.6) for adhesions, and 27.6% (95% CI
[(Fig._1)TD$FIG]
Fig. 1 – Flow diagram of the search strategy, screening, eligibility and inclusion criteria.
E U R O P E A N U R O L O G Y 7 1 ( 2 0 1 7 ) 7 9 0 – 8 0 7
792