















 698 844
698 844

rearrangements involving the
ERG
gene
[3,4], and genomic
deletion of the
PTEN
tumor suppressor gene
[4] .ERG
rearrangements have been observed in approximately half
of all PCas occurring in EA men, and are not associated with
adverse outcomes in most studies
[5]. By contrast, PTEN loss
has a strong association with adverse outcomes in predomi-
nantly EA cohorts, in which genomic deletion of PTEN occurs
in 20–50% of primary PCas
[6] .Interestingly, PTEN loss is two
to three times more common among
ERG
-rearranged tumors
in EA cohorts and may modify the association between PTEN
and lethal disease
[6] .Although African-American (AA) men have the highest
PCa incidence and mortality, the relative prevalence of
molecular PCa subtypes in the AA population is only
beginning to be elucidated. It is clear that
ERG
rearrange-
ment is significantly less common in the AA population
[7,8]. However, the relative rate of PTEN loss in AA PCa has
only been examined in a few small cohorts
[8–10]. In
addition, it is unknown whether
ERG
rearrangement and/or
PTEN loss are prognostic in AA PCa since most large cohorts
with clinical follow-up information studied to date are
predominantly EA men.
Because PTEN loss is more prevalent among
ERG
-
rearranged cases in EA PCa, and
ERG
rearrangement occurs
less commonly in AA compared to EA PCa, we hypothesized
that PTEN loss may be less frequent in AA PCa. We further
hypothesized that these molecular alterations, when
present in AA men, would have similar associations with
cancer-specific outcomes to those observed in EA men. To
test our hypotheses, we assessed tumor PTEN and ERG
status among self-identified EA and AA men who under-
went radical prostatectomy (RP) at our institution with
long-term clinical follow-up.
Following institutional review board approval, PTEN and
ERG status was assessed by immunohistochemistry in three
institutional tissue microarray (TMA) sets (Supplementary
methods). TMA 1 was derived specifically to test the
aforementioned hypotheses; grade-matched EA and AA
subjects were selected among all men with available tissue
and clinical follow-up who underwent RP from 1995 to
2005. TMA 2 included a nested case-control study
comparing men with and without biochemical recurrence
who underwent RP from 1993 to 2001. TMA 3 included
consecutive RPs from 2000 to 2004 not included in the
previous microarrays; subjects with Gleason score
>
6 were
specifically selected, as in previous studies, owing to their
higher risk of recurrence and metastasis, with the aim of
evaluating the association of these genomic risk factors
with the most clinically relevant cancers
[10] .Because TMA
2 and 3 were not designed explicitly for comparison by race,
and the RP population at our institution has been
predominantly EA, all three TMAs cumulatively ultimately
yielded 936 EA men with available PTEN/ERG status and
clinical follow-up (Supplementary Table 1), compared to
169 AA men. To ensure genomic differences by race were
not confounded by tumor grade or TMA design, AA men
were matched by Gleason score and microarray to eligible
EA men to yield 169 EA men for the study population. The
index tumor from each case was sampled in triplicate or
quadruplicate on each TMA and assessed using genetically
validated immunohistochemistry assays
[6](Supplementary
methods, Supplementary Fig. 1).
The matched AA and EA populations were not signifi-
cantly different in terms of pathologic grade and stage at
prostatectomy
( Table 1). The median follow-up among
those who did not experience biochemical recurrence (BCR)
was 6 yr (interquartile range 2–11). The 5-yr incidence of
BCR was 44% in AA men compared to 36% in EA men
( Table 1 ), while metastatic disease was rare in both
populations (7% in AA vs 8% in EA men at 5 yr;
Supplementary Fig. 2). Consistent with our hypothesis,
PTEN loss (18% in AA vs 34% in EA men;
p
= 0.001) and ERG
expression (25% in AA vs 52% in EA men;
p
<
0.001) were
significantly less prevalent in the AA population. Notably,
PTEN loss was observed in 14 of 43 (33%) ERG-positive
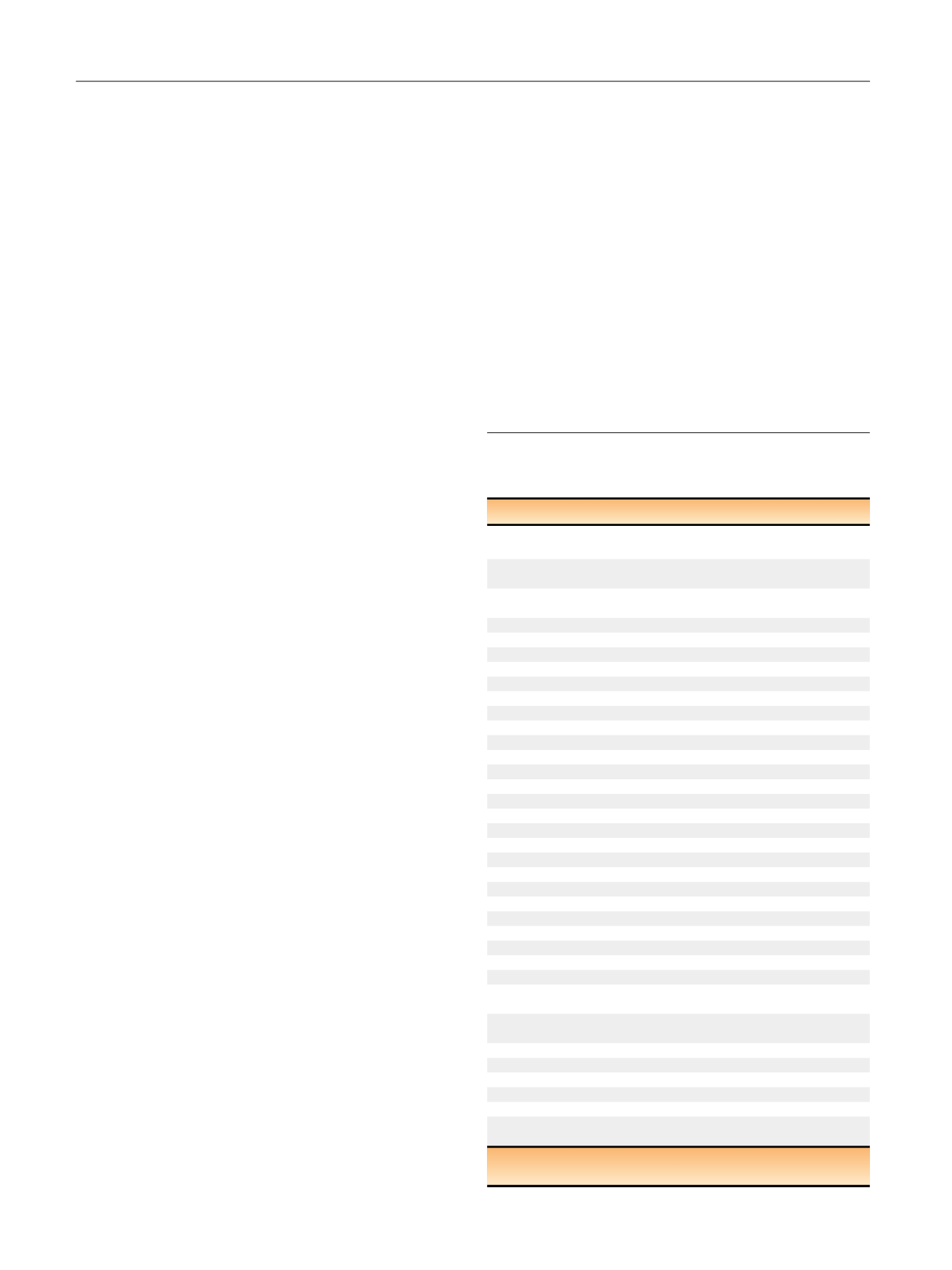
Table 1 – Clinicopathologic characteristics and PTEN/ERG status for
the matched African-American (AA) and European-American (EA)
cohort
Variable
AA (
n
= 169)
EA (
n
= 169)
p
value
Median age,
yr (IQR)
58 (53–62)
61 (56–65)
<
0.001
Median year of
surgery (IQR)
2001 (1998–2002) 2001 (1998–2002)
0.98
Median PSA,
ng/ml (IQR)
8.3 (5.8–13.1)
6.0 (4.7–8.3)
<
0.001
Clinical stage,
n
(%)
T1c
120 (71)
103 (61)
0.14
T2a
32 (19)
41 (24)
T2b
17 (10)
25 (15)
Biopsy grade group,
n
(%)
1 (GS 6)
91 (54)
92 (54)
0.99
2 (GS 3 + 4)
41 (24)
37 (22)
3 (GS 4 + 3)
23 (14)
25 (15)
4 (GS 8)
11 (6.5)
12 (7.1)
5 (GS 9–10)
3 (1.8)
3 (1.8)
RP grade group,
n
(%)
1 (GS 6)
43 (25)
43 (25)
0.99
2 (GS 3 + 4)
63 (37)
63 (37)
3 (GS 4 + 3)
31 (18)
31 (18)
4 (GS 8)
23 (14)
23 (14)
5 (GS 9–10)
9 (5)
9 (5.3)
Pathologic stage,
n
(%)
T2N0
72 (43)
76 (45)
0.7
T3aN0
67 (40)
59 (35)
T3bN0
18 (11)
17 (10)
N1
12 (7)
17 (10)
Tissue microarray,
n
(%)
1
110 (65)
110 (65)
0.99
2
36 (21)
36 (21)
3
23 (14)
23 (14)
Biochemical
recurrence (
n
)
68
67
5-yr biochemical
recurrence (%)
44
36
Metastasis (
n
)
19
20
5-yr metastasis (%)
7
8
PCa death (
n
)
10
8
5-yr PCa death (%)
1
1
PTEN loss,
n
(%)
31 (18)
57 (34)
0.001
ERG expression,
n
(%)
43 (25)
87 (52)
<
0.001
IQR = interquartile range; PSA = prostate-specific antigen; GS = Gleason
score; RP = radical prostatectomy; PCa = prostate cancer.
E U R O P E A N U R O L O G Y 7 1 ( 2 0 1 7 ) 6 9 7 – 7 0 0
698