















 745 844
745 844

confounded by different genetic backgrounds between the
two comparison groups).
Thirdly, our results confirmed the association of muta-
tions with short survival time
[10,12–14,16,17,19] ,provid-
ed critical data for association of mutations with age of
PCa-specific death, and importantly, for the first time,
demonstrated a dose-response relationship between mu-
tation carrier rate and age of death, as well as time to death.
We found mutation carrier rate is highest among lethal PCa
patients who died 60 yr (10.00%) or died within 5 yr after
diagnosis of PCa (12.26%), and lowest among patients who
died of PCa
>
75 yr (2.97%) or died
>
10 yr after diagnosis of
PCa (0.98%). The mutation frequencies of the latter groups of
lethal PCa patients were similar to those with localized PCa
(1.23%). These results suggest that not all lethal PCa patients
have
[16_TD$DIFF]
a
[17_TD$DIFF]
similar genetic basis and mutations in these three
genes increase the risk for the most lethal form of PCa—
dying younger and faster.
Our results, together with previous findings, may have
important clinical implications. According to the National
Comprehensive Cancer network guideline for PCa early
detection, it is recommended to inquire about known
BRCA1/2
mutations in the family
[30]. We propose to expand
the inquiry to include whether there is a family member
who died of PCa before age 75 yr. If they meet either
condition, a genetic test of
BRCA1/2
and
ATM
is recom-
mended. Another clinical implication of our findings is to
consider inclusion of mutation carrier status as another
important factor for decision making in active surveillance,
although genetic studies specifically in active surveillance
cohorts
[18_TD$DIFF]
are needed for such indication. Mutation carriers
may consider other types of interventional treatment.
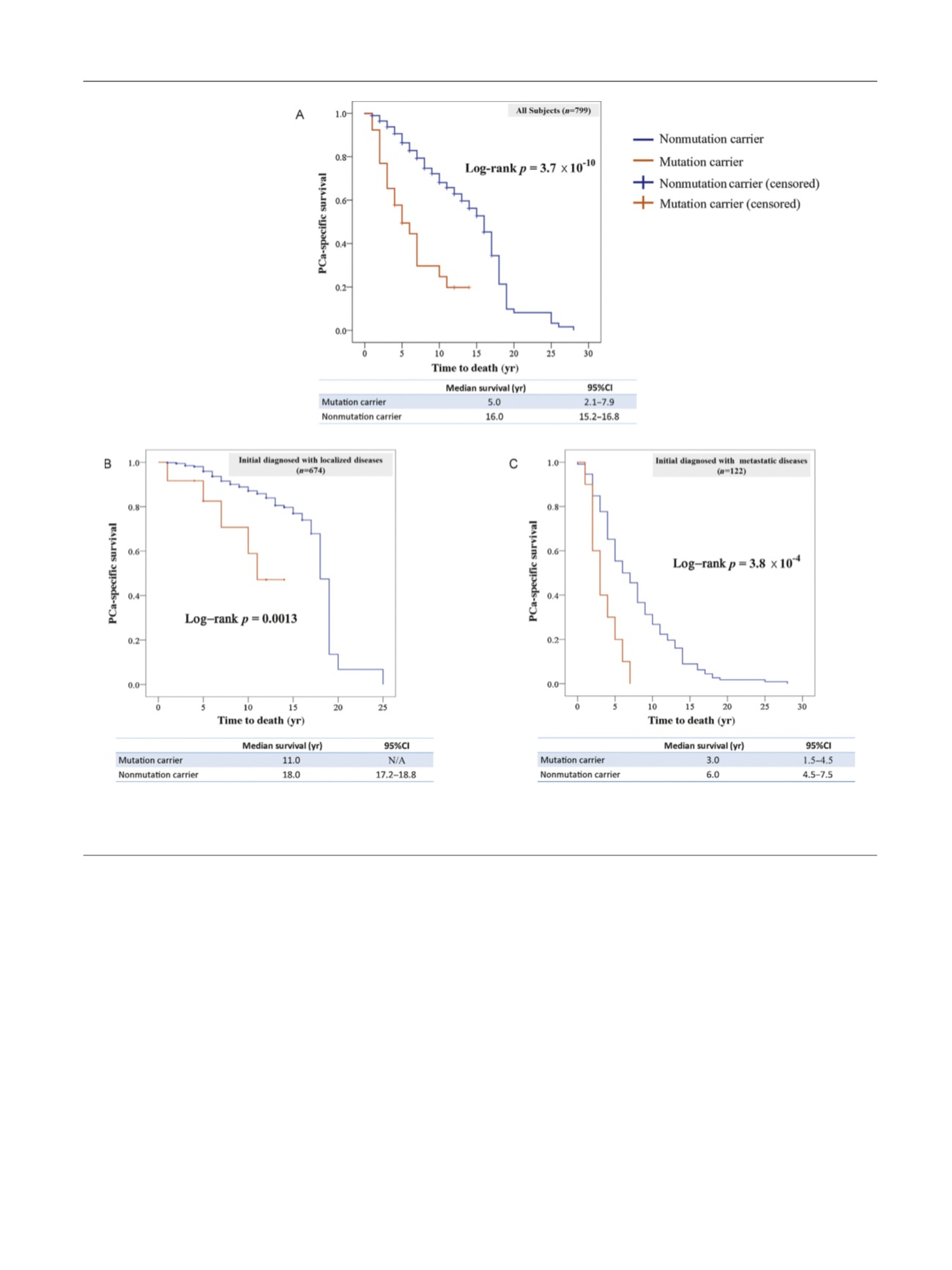
[(Fig._2)TD$FIG]
Fig. 2 – Kaplan-Meier survival curves for mutation carriers and noncarriers (A) in the entire study cohort, (B) in patients diagnosed with localized
prostate cancer at time of diagnosis, and (C) in the patients diagnosed with metastatic prostate cancer at time of diagnosis.
PCa = prostate cancer.
E U R O P E A N U R O L O G Y 7 1 ( 2 0 1 7 ) 7 4 0 – 7 4 7
745