















 809 844
809 844

bladder wall is caused by external peritoneal infiltration
( Fig. 1). As rightly assessed by the authors, transurethral
resection surgery is ineffective
[1]. Proper completion of
partial cystectomy need to consider uterine involvement by
external endometriosis which is a quasi-constant compo-
nent of the lesion
( Fig. 1) and has to be treated without
impairing uterine function; second, intrinsic ureteral
endometriosis due to contiguous extension of bladder
disease requires a resection-reimplantation procedure, but
fortunately this situation is rare. Extrinsic ureteral disease,
often due to remote associated lesions (posterior and/or
lateral), is mainly treated using conservative surgery of the
ureter. In symptomatic bladder disease surgery can be
envisaged in several ways. The first is complete surgery: a
bladder phase, and completed at the same time—or not—via
resection of posterior or lateral lesions, which are always
associated
[5] .The alternative strategy, called
site-specific
surgery
, is to perform only the anterior procedure and not to
treat posterior lesions when they are important or require
difficult procedures, for example when the disease involves
the digestive tract. Again, preoperative imaging is essential
for a comprehensive description of the lesions, which will
govern the surgery type and principle.
The management plan must be conceived as a
comprehensive and long-term strategy that considers
fertility and childbearing; the excellent review by
Maggiore et al
[1]provides much useful information for
reflection, but few clear-cut guidelines. Endometriosis
surgery represents a risk to the uterus and adnexa, and
complications of surgery are also a cause of infertility.
Thus, the benefit-to-risk ratio for surgery versus medical
treatment should be carefully considered. One of the main
characteristics of symptoms related to DIE lesions is that
they dramatically respond to therapeutic amenorrhea
[6]. Therapeutic amenorrhea is one of the key approaches
for treatment of endometriosis in general, and bladder
endometriosis in particular. It can be achieved simply via
continuous administration of combined hormonal contra-
ceptives. Infertility, which may be closely related to
endometriosis, including bladder endometriosis, can be
properly treated via assisted reproductive techniques,
thus bypassing the need for surgery
[1].
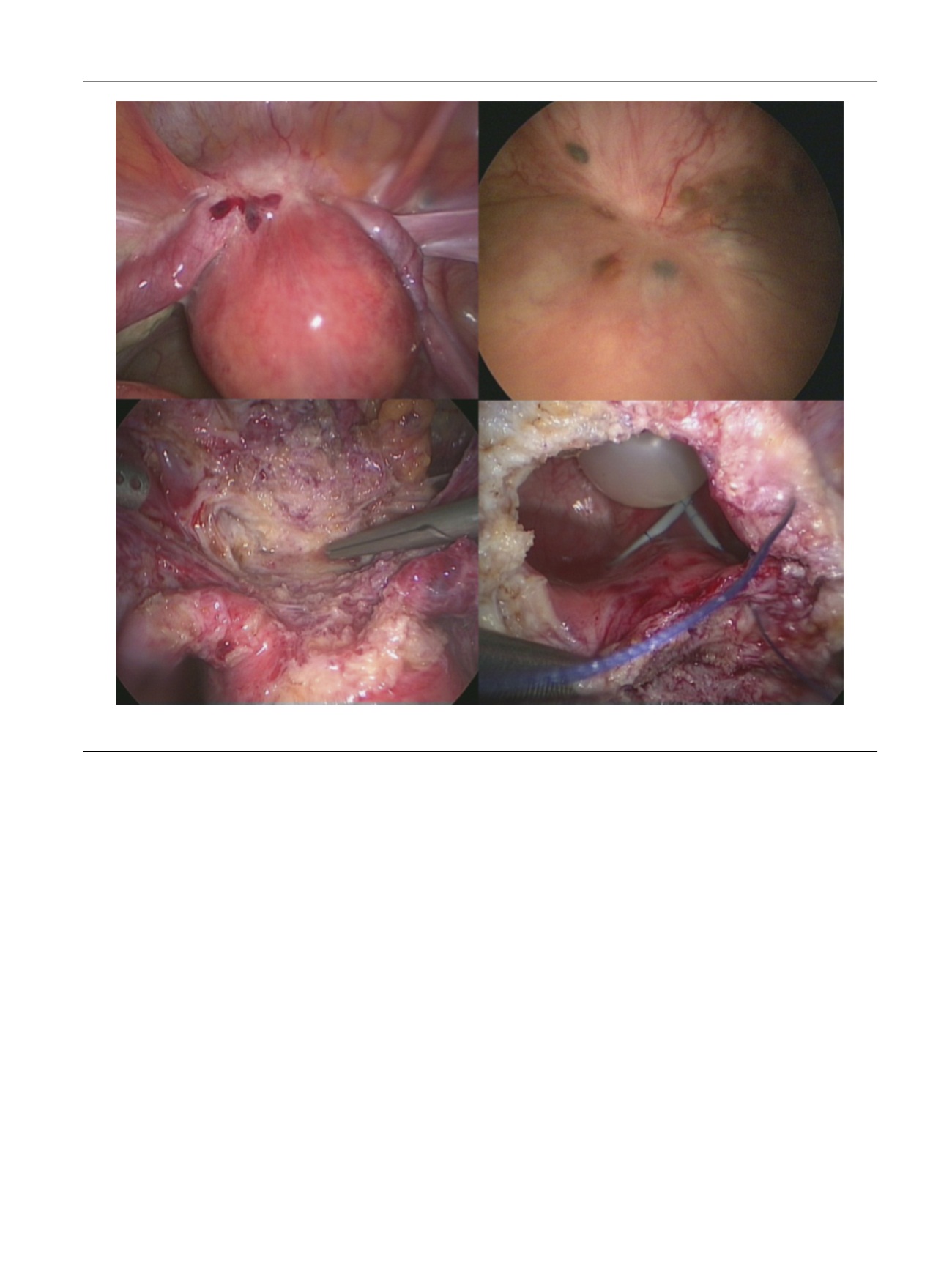
[(Fig._1)TD$FIG]
Fig. 1 – Extensive bladder endometriosis with detrusor and mucosal involvement and associated uterine infiltration.
E U R O P E A N U R O L O G Y 7 1 ( 2 0 1 7 ) 8 0 8 – 8 1 0
809